Acute Pancreatitis (AP) is an acute pancreatic inflammatory disorder caused by intracellular activation of pancreatic digestive enzymes.
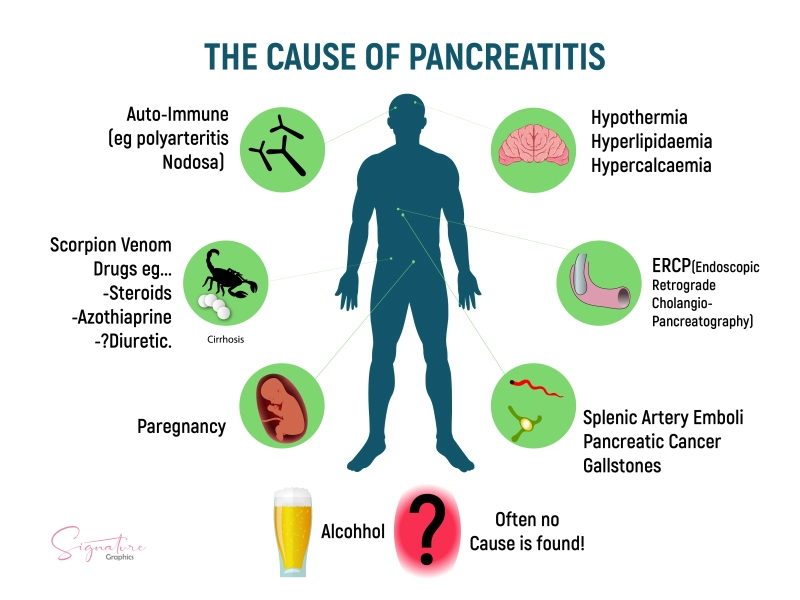
Causes of Pancreatitis
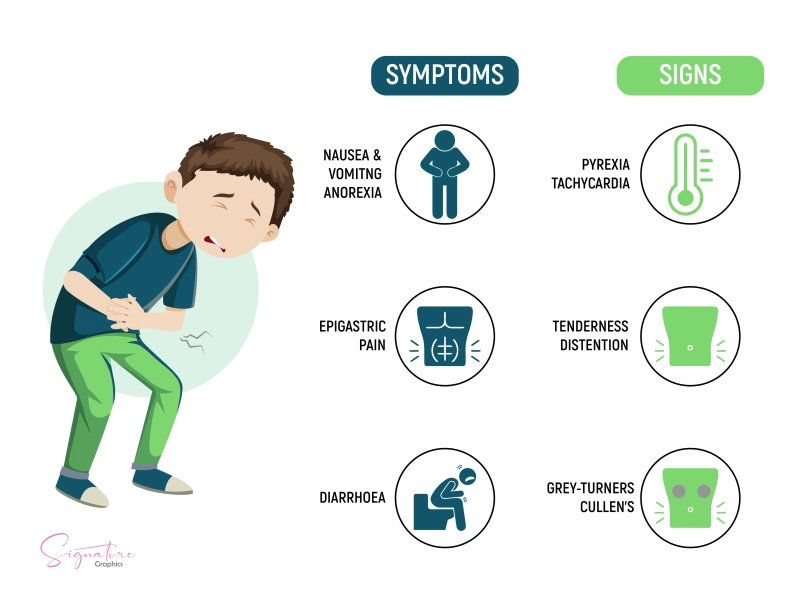
Signs and Symptoms of Pancreatitis

Gastric Ulcers | Causes, Symptoms, Complications & Treatments
Gastric ulcers are defined as a break in the mucosal barrier of the stomach lining that penetrates through the muscularis mucosa and is larger than...