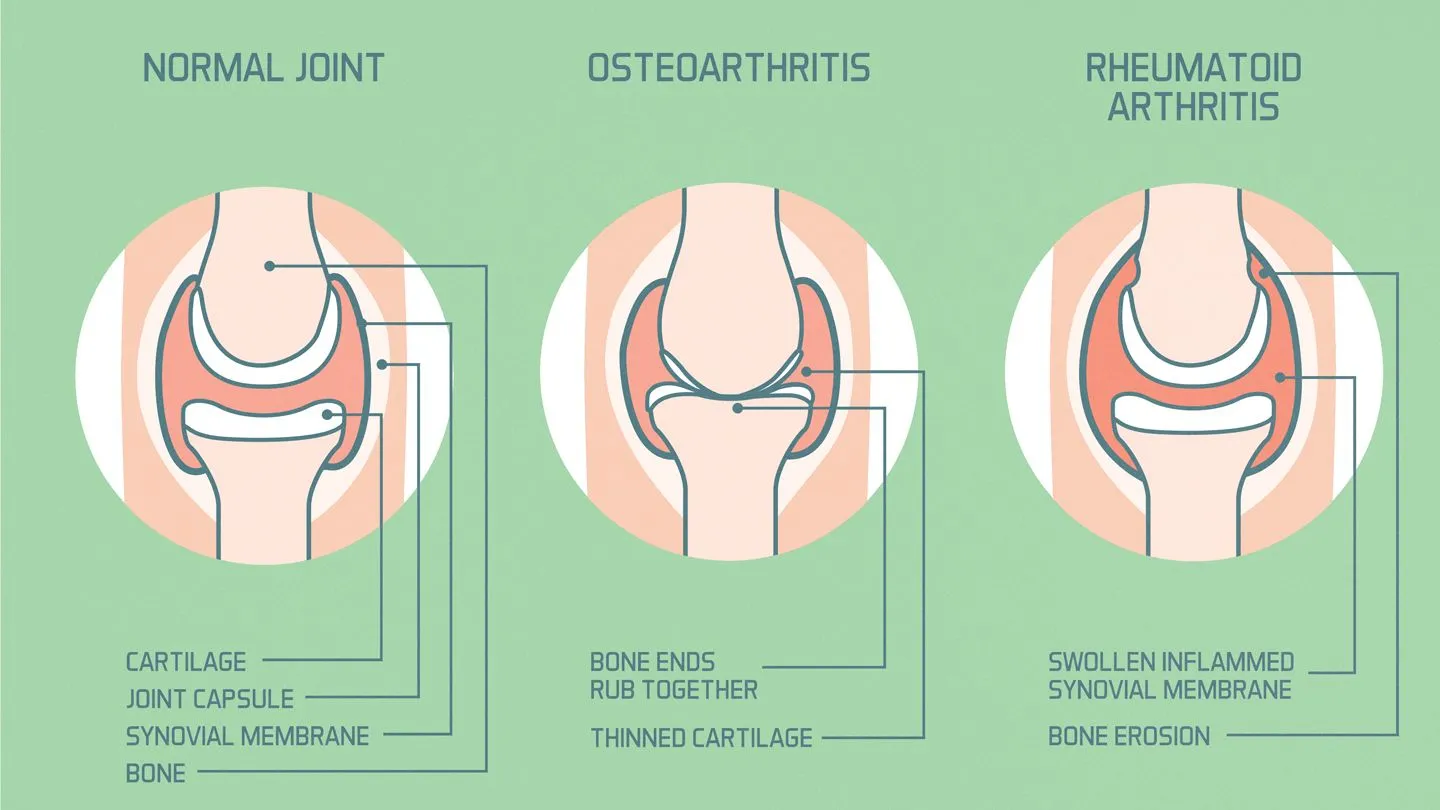
Rheumatoid arthritis is a progressive, chronic, and degenerative autoimmune inflammatory disease that is primarily characterized by synovitis.
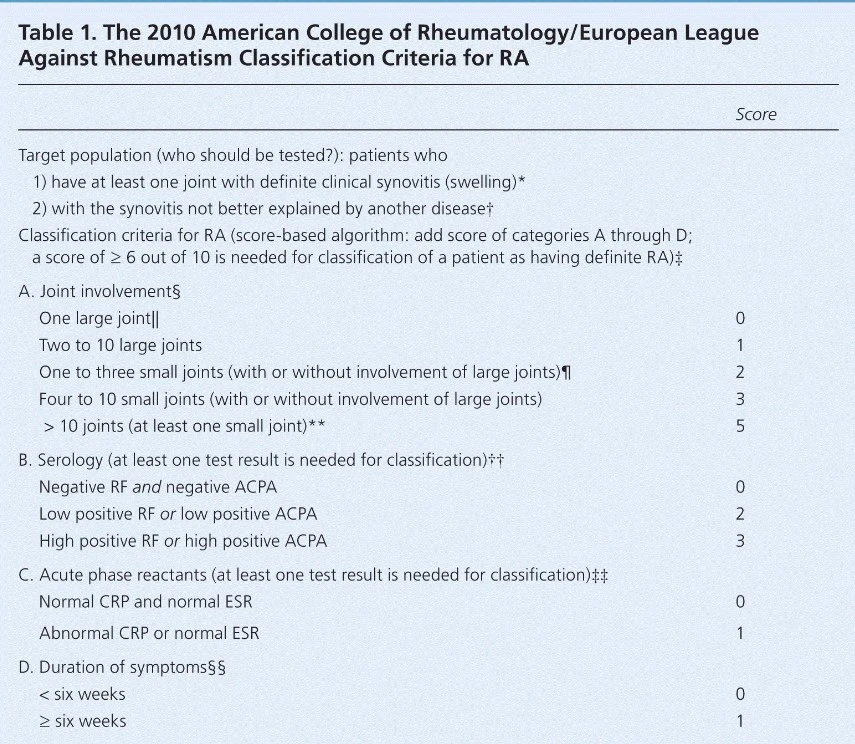
The 2010 American College of Rheumatology/European League Against Rheumatism Classification Criteria for RA
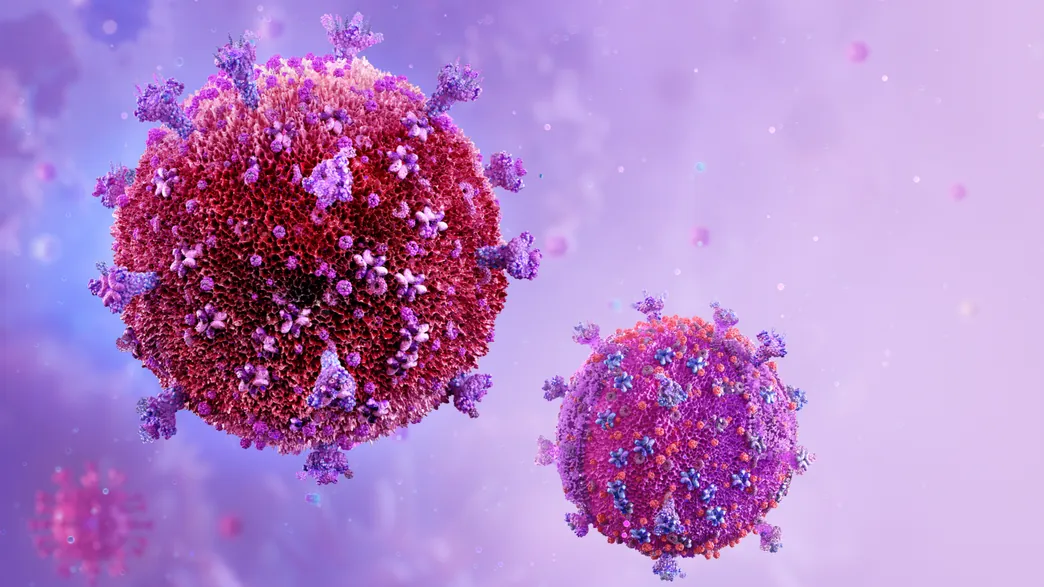
Human immunodeficiency virus (HIV) is an enveloped retrovirus … There are four main stages of HIV infection.

SAPHO syndrome is a chronic immune-mediated condition that affects the skin, joints, and bones.
Good's syndrome is a rare adult-onset thymoma-related immunodeficiency with an unknown cause.